AI in Radiation Oncology versus Palliative Care: The Rich Get Richer
By Roy F Rada, MD, PhD
Placed on LinkedIn: August 2025
Keywords: Large Language Models, Generative AI, Healthcare, Radiation Oncology, Palliative Care, Rich get Richer
Rich grow richer and poor fall further behind. Image generated by Microsoft CoPilot for Roy Rada
Executive Summary
The history of computer applications in healthcare supports the famous Rich get Richer phenomenon. New investments in digital information systems in healthcare have typically gone into areas that most depend on digital information. This essay focuses on two application areas, radiation oncology and palliative care, which sit at opposite extremes of the capital spectrum. Radiation oncology attracts massive AI investment but palliative care not. Could things be different?
AI and healthcare have impacted one another since the beginning of AI. Traditionally, the branches of healthcare most dependent on digitized information benefited the most from AI. Do the latest advances in natural language processing impact the trajectory? Since Large Language Models (LLMs) exploit free-form text, do they open opportunities for branches of healthcare traditionally reliant on human-human interaction? Or will the areas that get the most investment now be the ones that get the most investment in the future, as a continuation of the famous aphorism 'the rich get richer, while the poor get poorer'.
The history of computer applications in healthcare supports the famous "Rich get Richer" phenomenon. New investments in digital information systems in healthcare have typically gone into areas that most depend on digital information. Historically, the first healthcare computer investments were in rich areas, first accounting and then radiology and pathology. Healthcare and AI illustrate that the rich get richer. This essay next focuses on two application areas, radiation oncology and palliative care, which sit at opposite extremes of the capital spectrum.
Radiation oncology is one of three oncology branches, the other two being medical and surgical oncology. In preparing a radiotherapy treatment plan, the doctors acquire images, segment the target, and plan doses to kill cancer cells. Radiomics is a method to quantitatively analyze medical images to uncover tumoral patterns not appreciated by the naked eye and to support personalized therapy. Doctors try to predict outcomes based on both radiomics and genomics. In the delivery of radiation, the team monitors patient changes and adapts treatment. Changing radiation based on patient motion occurs in real-time under computer control. Radiation oncology relies on massive amounts of digital information and repetitive tasks -- 'Big Data' incarnate.
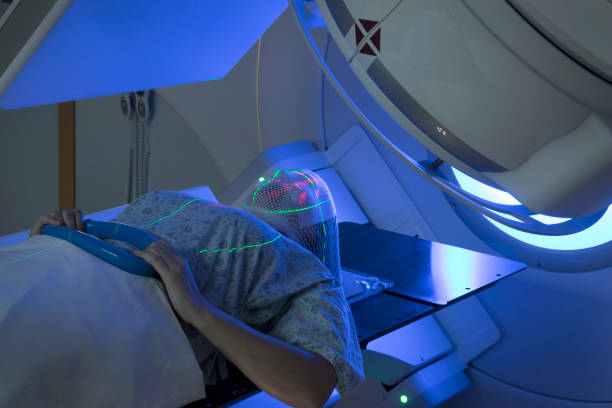
Patient receiving radiation for brain cancer (public domain image)
Radiation oncology is ripe for AI applications. Radiation oncologists appreciate AI's impact and say that AI revolutionizes radiation therapy. AI is transformative at every step of the radiation oncology process.
Palliative Medicine differs sharply from Radiation Oncology. The World Health Organization says that palliative care improves the quality of life of patients and their families who are facing life-threatening illness, through the prevention and relief of suffering whether physical, psychosocial, or spiritual. Diseases benefiting from palliative medicine include cancer, heart failure, and stroke. Nevertheless, only a small fraction of people who need palliative care currently get it. Health insurance underfunds palliative care, and hospitals, at a loss to themselves, provide much of the overall cost of palliative care.
Family holding hands of dying patient. Image courtesy of MD Anderson Cancer Center
Palliative care uses AI less than radiation oncology. Grant and patent activity evidences the divide. The US National Institutes of Health (NIH) provides 'Research Portfolio Online Reporting Tools' for a repository of both intramural and extramural NIH-funded research projects and patents resulting from NIH funding. A search in early 2025 on this NIH repository for 'radiation oncology' AND 'artificial intelligence' returned 68 active projects linked to 60 patents. A search on 'palliative care' AND 'artificial intelligence' retrieved 10 active projects and 0 patents. Radiation oncology is 'richer' than palliative medicine.
LLMs can support palliative care:
An LLM for patient mental health showed that the LLM-system responds like a professional mental health counselor.
For the doctor, an LLM inferred wishes of mentally incapacitated patients based on prior records.
Mortality and pain are major concerns of palliative care. LLMs can forecast mortality and monitor pain.
For predicting mortality, one project uses traditional machine learning on structured data sets, while another project uses an LLM that reads unstructured medical records. Both projects had similar accuracy. However, since the LLM approach works on unstructured natural language, it lends itself more readily to extensions and diffusion into Electronic Health Records systems.
A successful LLM roll-out must fit into the workflow. The surge of interest in expert systems in the 1980s bares comparison to the surge of interest in LLMs. The 1980s MYCIN expert system was as good as expert physicians in its problem area of bacteremia, and it offered recency, accuracy, coherence, and transparency confirmed by clinical trials. However, to use MYCIN, the physician needed to access a separate, stand-alone application and re-enter patient information into that application which took enough time that the cost/benefit ratio was too high for the physician. MYCIN did not fit into the workflow and failed commercially.
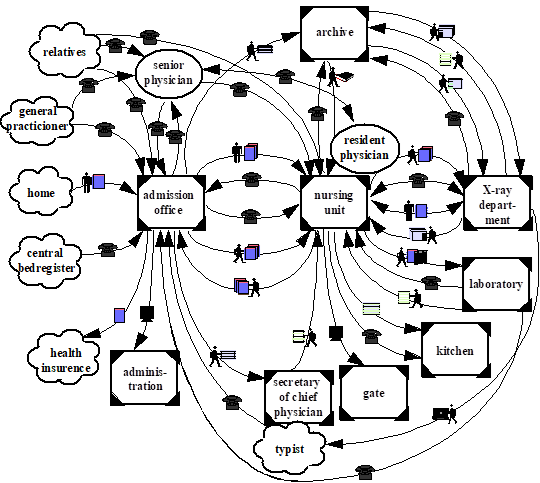
Image courtesy Krabbel et al, (1996) "Participation of User Groups: Hospital Information System" Proc Participatory Design.
Workflow systems rely on roles defined as functions with rules for passing messages among roles. LLMs can mediate between roles and between a role and the rules of that role. In radiation oncology, automation of workflow with the support of LLMs is advanced, but not in palliative care. However, palliative care could lend itself to automation of workflow.
A hospice care system, which is the ultimate example of palliative care, suits LLM integration into the workflow. The system could represent the roles of the interdisciplinary team and the roles of patients and their family. Consider dignity therapy. Dignity therapy helps patients reflect on end-of-life issues. The patient receives nine standard questions which guide a conversation. The dialog is recorded, transcribed, and edited into a legacy document for the patient to use in implementing the last steps of life. However, dignity therapy is underutilized due to a lack of trained staff to help. With an LLM-automated social worker, patients could develop their dignity document.
Radiation oncology relies on Big Data, attracts investment, and uses AI extensively. Palliative care relies on human-human interaction, attracts little capital, and uses AI sparingly. Radiation oncology is rich and getting richer. Palliative care is poor and getting poorer. The betting AI entrepreneur invests in radiation oncology rather than palliative care, but does it have to be that way?
Palliative care does not process vast amounts of information in real-time, as radiation oncology does. Palliative care relies on natural language communication. As death approaches, the roles of palliative care and natural language communication increase. LLMs could support palliative care applications both clinician-facing and patient-facing across every phase of the clinician and patient experience. But that's not where the money is.
Footnote
This essay is based on Roy Rada's "Generative AI and Healthcare: Brief Survey" published by the 'IEEE Computer Society' in its flagship magazine Computer, July 2025, pages 153-156.